Extended shallow stops Increases DCS
Hello,
I am late to respond to this thread. Sadly there appears to be a few mistakes in the opinions offered above.
Here are some facts to consider:
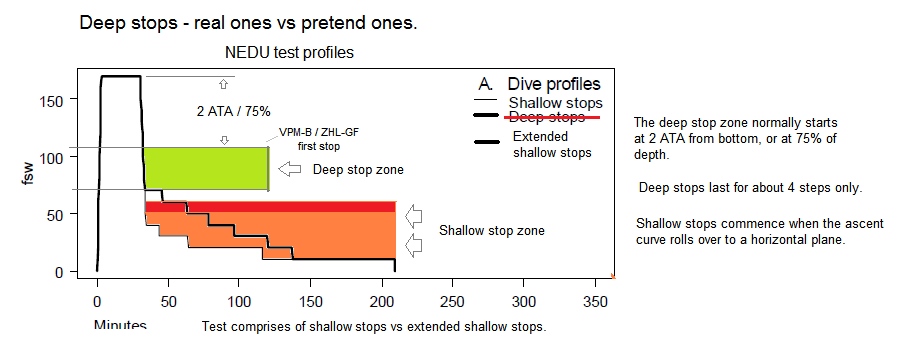
1/ The Nedu test did NOT test deep stops. What that really tested was "Extended time shallow stops" which is then miss represented to be deep stops.
The test profiles comprise of shallow stop segments only. The VPM / RGBM / RD / DIR stops were never applied or used in the test.
Beware: The "longer and shallower" style ascent being recommended, is the same type that produced the increased DCS in this test. Repeating myself .... higher risk came from extended shallow stops - not deep stops.
2/ The profiles and plans in the test come from experimental Nedu designs (both shallow stop models), and do not represent anything we use today.

 3/
3/ These tests profiles do NOT have high supersaturation. In fact they are the opposite, and from a gas pressure perspective, these test profiles offered a very low risk. The current "plausible explanations" given that have attributed the causes to supersaturation, are plain wrong. The underlying cause of injury appears to be with other factors.


Our latest V-Planner and MultiDeco programs, give diagrams that show supersaturation throughout the ascents (shown in the diagram above). It's a new and unique view on deco diving and risk. Press the bubble icon on the right side. Make some plans and decide for yourself.
More diagrams taking a close look at this Nedu test are here:
nedu test review



")

