Now I have to ask, What is a technical diver? Is it anybody who dives to do a specific job underwater (such as maintaining a drilling rig), or is it anybody who does decompression diving? If the former, then what do you call a diver who does decompression diving but isn't a technical diver?
General definitions:
Recreational Diver: A 'sport' diver whose qualifications/agency recommended limitations limit them to no greater than 40m/130ft total linear distance from the surface, no-decompression, no overhead environment beyond the light-zone, no gas-switching during a dive, no nitrox >40%.
PADI, SSI, NAUI etc... all provide 'recreational diver' programs. They clearly differentiate these from more advanced, 'technical' syllabus.
Technical Diver: A 'sport' diver whose qualifications/capability exceed recreational diving limits, particularly in regard to conducting decompression dives, including the use of multiple/mixed gasses for accelerated decompression and extended depth beyond the PPO2 or narcotic limits of air or enriched air. Depth limits exceed recreational diving maximums, tending to be limited by the characteristics of the mixed gasses used. Not limited to <40% O2. May dive in overhead environments beyond the light zone.
Technical diving is often considered (as an over-arching term) to include accelerated deco, cave and advanced wreck diving...either individually, or in combination. Many divers also consider CCR (closed circuit rebreather) diving to be 'technical' - although it does not strictly necessitate the use of gasses, procedures or limitations described above.
Technical diving is also dependent on the correct application of the skills, procedures and preparations that are taught as effective risk mitigation factors for the scope of diving undertaken. Doing a dive beyond recreational limits, but using recreational diving equipment and procedures does not make it technical diving. Thus, there is also a 'mindset' or psychological differentiation between technical divers and 'aggressive/extreme' recreational divers - one group seek to
mitigate anticipated risks... the other group is happy to
accept those anticipated risks.... or is just ignorant of them. The only logical term for such practices would be
Stupid Diving, although the divers who engage in it would love to have you believe otherwise...
Commercial Diver: A 'working' diver who is employed to conduct various forms of construction, maintenance and salvage underwater. Training/function/role extends from shallow SCUBA dives, surface supplied air sources, surface (chamber) decompression... through to extended saturation diving from a working 'bell' at great depths underwater.
Sport Diving: Scuba diving that is not commercial, scientific (biology, archaeology etc) or military in application. Generally viewed as 'fun' diving, but also includes professional work, such as recreational/technical scuba instructors, underwater photographers and videographers (not otherwise acting in a scientific role).
In some cases the exact differentiation between 'rec' and 'tec' may be confused... some agencies allow 'lite' decompression within the recreational training system (i.e. CMAS and BSAC). Others allow the use of normoxic He mixes ('recreational trimix') for narcosis reduction within 'recreational' diving ranges (typically 30m/100' - 40m/130'). CCR diving is being increasingly marketed to the 'recreational' market.
Note: these
general definitions are based upon training syllabus and the related agency recommended limitations amongst the 'bigger' scuba-training agencies. It does not reflect the 'actual diving' necessarily done by divers - some people view recommended limits as entirely optional. Divers who were trained prior to the 1980's were limited by modern training syllabus and, likewise, may have a greater scope (more blurring between rec and tec) than modern generations.
It seems to me that what raises your ppO2 is going deep. If you're in the process of ascending, how would you go from having a lower ppO2 to a higher ppO2? For example, let's say you go to a depth that raises your ppO2 to 1.4. You swim around for awhile. Then you decide to decompress. How does your ppO2 now increase to 1.6 for decompression purposes? If you ascend, your ppO2 will drop, not increase.
You change gas!

Technical divers... doing 'accelerated' decompression will move onto richer O2 mixes during ascent/deco schedule.
My (limited) understanding is that a fast compartment will saturate more quickly than a slow compartment. Thus, if a fast compartment is now a super-fast compartment, you'll reach your NDL sooner. But a faster compartment will also off-gas more quickly, so you would not have to decompress for as long. So with Helium you would get more saturated more quickly (requiring longer decompression times), but be able to decompress more quickly (requiring shorter decompression times). The question is, what is the net--longer or shorter decompression for a dive with Helium?
The difference lies in the range of tissue compartments that are saturated. Not only speed of saturation, but (due to small molecular size) the degree to which He can saturate into the body. Whilst this is dictated by the exact depth/profile of the dive, along with the exact mixture used - the end result is that He gasses don't permit drastically shorter decompression. In some cases, the deco might be longer.
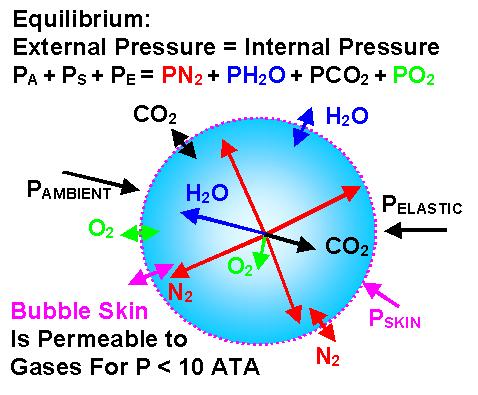
This doesn't sound quite right to my neophyte mind. I doubt that oxygen absorbed into tissues is going to decrease the formation of nitrogen bubbles on ascent. For one thing, the oxygen is going to get metabolized quickly, so won't stay absorbed in tissues for long. For another, I don't think gases behave that way. One gas coming out of solution I don't believe is affected by the presence of another gas in the same solution.
But inert gas contained in a bubble isn't in the same solution as the gasses saturated into a liquid surrounding that bubble.
The key to off-gassing is the differential between gas partial pressures in varying states of the cardio-vascular system. The pressure
differential between gasses contained in the lungs and those in solution in the blood passing the lung (blood-lung barrier). The
differential between gasses saturated in tissues and those in the blood that flush the tissues. The
differential between gas trying to form in a bubble and those in the liquid surrounding it.