Okay, I've sat on this discussion for a while now, but now will talk a bit about what I, an outsider with no rebreather experience, see as deficiencies for the rebreathers. Here are the ones I've identified during these discussions.
--High on my list is a lack of a CO2 indicator. Rebreathers have oxygen indicators, most times redundant (or triple redundant), but nothing to indicate carbon dioxide poisoning potential. Both can kill, and recent deaths (there have been several) underline this deficiency.
--Continued buoyancy problems. Because of the breathing loop, rebreathers are positively buoyant, but if they flood, there is an instant negative buoyancy. When I went over a scenario about using a buddy line with one rebreather user, he stated that he would not be tied to another rebreather diver because of this negative buoyancy, and the increased work (with a resulting potential of CO2 poisoning for the rescue diver, who is also using a rebreather). If this is true of all rebreather divers, then all rebreather divers dive virtually solo.
--Rebreather technology for removing CO2 is still back where it was in Hans Hass' days. There has got to be a better way (and apparently there is at least one newer alternative).
--Lack of automatic redundency. There is one loop, and the diver is left to determine when to switch to OC. The diver is already in a condition of CO2 poisoning, with resultant lethargy and confusion, yet has to make this determination on his or her own. If someone wants me (or other experienced OC divers) to think about rebreathers, then they need to sense when the scrubber no longer is working, and make the switch automatically. Some rebreather divers may cringe at this, and say that they depend upon their training and monitoring of their own physiology to do this, but that is not a reliable way of coping with this safety-critical failure mode. There should be no single-point safety critical failure potentials in a life support system.
Observations
Rebreather divers rely upon their training and checklists. This training is extensive, and the divers are told by instructors that the rebreathers are trying to kill them. They need to be hyper-vigilant about their own bodily reactions, even though those reactions themselves compromise this ability.
As a safety professional, with over 35 years experience in both occupational safety and product safety, we rely upon a concept called the "
Hierarchy of Controls." Those controls go from the most effective to least effective control measures, and look like this:
Elimination > Substitution > Engineering Controls > Administrative Controls > Personal Protective Equipment
Note that training, the use of checklists, and procedures are all administrative controls. They are effective as long as the followed without exception; but there are always exceptions.
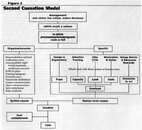
There are several different models of accident causation. One part of one is by
Dan Peterson, his Second Causation Model. Note that it states that "Management sets vision, has values, makes decisions." So too do companies who design life support systems, and the instructors who teach divers to use them. Rebreather divers have created their own culture, which is somewhat different from that of OC divers. But in doing so, they have put some blinders on concerning the equipment that they are using (rebreathers). Because of this, the rebreather diving community is going to have to change its entire outlook in order to make rebreathers better. This includes new engineering designs, which overcome the limitations I've outlined above.
Note that Mr. Peterson talks also about "Traps." In my view, the rebreather of today has many of these traps, and they need to be eliminated. There is also a person's "capacity," with a "load," in a "state." Today's rebreather diver is asked to ascertain his own state, in a high load situation, with a diminished capacity. To me, that is simply not acceptable.
SeaRat
John C. Ratliff, CSP, CIH, MSPH
NAUI #2710 (retired)
(CSP =
Certified Safety Professional; CIH =
Certified Industrial Hygienist)



")
