Just a quick lesson in medical diagnosis. There are two types of figuring out what a patient has for a diagnosis. You can "rule in" where you present and based on history, exam, labs, and imaging you have a single diagnosis. Or, you can "rule out" for a disease where you have something and based on a screening test you either might have one of a number of things or completely don't have the condition.
Let's go back to my chest pain analogy. If you come to the ER with chest pain I'm going to do an EKG. Let's just say by history what you describe is classic angina. Chest pressure worse with exertion and relived by rest. To further suggest cardiac cause you received nitroglycerin and then pain got better. But your EKG is normal. Does that mean you don't have a narrowed artery in the heart causing your symptoms?
Given this scenario based on the EKG you haven ruled out for an acute heart attack. So you are not having actual cell death of the heart muscle. But there is stil a significant probability you still have heart disease in the form of a narrowed or stenotic artery. At this point you have ruled OUT for heart attack but have yet to rule IN for atherosclerotic heart disease.
So so we do the next step. The cardiologist does a stress test that is now positive for a blocked artery. You have now ruled IN for atherosclerotic heart disease. You now go to the cath lab and low and behold you have a 90% lesion and you get a stent.
But doctor, my EKG was normal. So how can I have heart disease. It's semantics. A myocardial infarction is a type of heart disease. But so is atherosclerotic heart disease. They have different definitions and different criteria for diagnosis and separate clinical criteria and treatments for both types of "heart disease". Not the same.
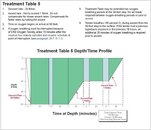
Let's take a diver who surfaced with some tingling in the arm. By definition it is either emergent DCI since the diver exited the water with symptoms. Or it is urgent since by definition numbness or paresthesia is neurologic DCI until proven otherwise. Now definitive therapy is Navy dive table 6 protocol until symptoms disappear. But the diver gets better with oxygen. At this point the diver has not yet ruled in, ie definitely has DCi. But getting better doesn't rule out DCI either. Quite the contrary. It has now increased the probability the diver has DCI since one would expect symptoms of DCI to improve with supplemental oxygen.
Now in the case of numbness you ruled out for DCI because by definition a true neurologic case DCI should have presented hours later. That is why when you feel better after oxygen you still require medical attention. As for the numbness, one could surmise medically you had a mild pinched nerve in the neck with radiculopathy that improved coincidentally while you rested and took oxygen. medically speaking you can't make the diagnosis definitively that it is for sure DCI because it is still probable that there is a chance it is something else.
Or you got very, very lucky and did not experience any permanent neurological damage from completely ignoring potentially serious DCI symptoms.
If if you go to the ER with chest pain and you are sent home with a diagnosis of heartburn that patient will tell a friend who complains of chest "don't worry, you have indigestion. Take some Tums and you'll be fine." Another patient goes to the ER and gets diagnosed with a heart attack. That patient tells his friend "You have to go to your doctor now. You might have heart disease."
When I say anecdotal experience doesn't count it's because in my experience patients loosely group their own experiences and then extrapolate that event to other similar conditions. Each individual situation is so unique you really, really can't make one experience fit all situations.
---------- Post added April 4th, 2015 at 12:45 PM ----------
Just thought of something waiting here in the airport.
Let's go back to my chest pain analogy. There is something we call pretest predictive value. If a young 20 years healthy fit individual presents to the ER with chest pain they have a low predictive suspicion for chest pain related to heart disease. More likely to be heartburn or indigestion. But if a over 60 out of shape diabetic smoker with previous history of a heart attack presents with classic chest pressure you have a very high predictive value it's heart related. But in either scenario if you give nitroglycerin for chest pain both patients might tell you they feel better. That's because indigestion might improve symptomatically with nitroglycerin too.
Going back lack to the oxygen issue. Take a diver with DCI symptoms but doesn't have DCI getting better with oxygen. No harm no foul. Take a diver with DCI symptoms who actually has DCI but whose symptoms get better with oxygen then thinks they are okay and they don't get proper care. Then hours later get a permanent injury when symptoms return. Actual harm. It's like the patient with chest pain who gets better with nitroglycerin. In the case of heartburn no harm no foul. If they are having a heart attack, start to feel better then leave the ER, possible dead patient.